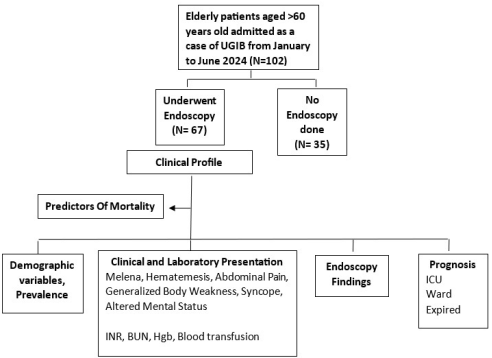
Background of the Study: Upper Gastrointestinal bleeding (UGIB) remains to be a significant clinical concern for geriatric patients due to their prolonged hospital stay and higher mortality and morbidity rates. The clinical profile of the geriatric patients are important aspects to consider, given that there is limited data in elderly population. Objective: The study is aimed to determine the clinical profile of elderly patients with UGIB admitted in a Tertiary Hospital from January 2024 to June 2024. Methods: This is a retrospective cohort study among elderly Filipino patients aged 60 years and above; admitted as UGIB and underwent esophagogastroduodenoscopy (EGD). Baseline Demographic, clinical presentation, laboratory results, endoscopic findings, prognosis and predictors of mortality were evaluated. Statistical analysis involved the application of Pearson’s chi-square, Fisher’s exact test, T-test and univariate and multivariate logistic regression analysis. Results: Among 102 admitted elderly patients with UGIB, 67 of them underwent EGD, thus were included in the study; 43 (64.18%) were male and 24 (35.82%) were female with the median age of 69.66 (±7.40) years. The prevalence rate of UGIB among elderly Filipino is 8.90%. 50 of those patients (74.63%) had comorbidities, the most common were: hypertension 38 (56.72%), diabetes mellitus 19 (28.36%) and chronic kidney diseases (13.43%). Patients presented mostly with melena (67.16%), generalized body weakness (53.73%) and 19.40% had abdominal pain. During endoscopy, (47.76%) was due to gastritis and gastric ulcer (19.40%). Mortality rate was higher in patients admitted at the ICU. No association was noted between the patients’ mortality and their sex, age, comorbidities, medications used, clinical findings, INR, BUN, hemoglobin, blood transfusion, and endoscopic findings. Conclusion: The present study reported that elderly patients with UGIB were male, with hypertension as the most common comorbidity. EGD findings showed gastritis as the most common cause of UGIB. Mortality rate is higher in patients admitted at the ICU. None of the variables showed significant differences in terms of predictors of mortality.
| Published in | International Journal of Gastroenterology (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijg.20250901.13 |
| Page(s) | 15-24 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Upper Gastrointestinal Bleed, Elderly, Clinical Profile, Melena, Predictors of Mortality
Number of Admissions | |
|---|---|
Patients >60 years old | 1445 |
Patients >60 years old admitted as UGIB | 102 |
Prevalence Rate | 8.9% |
Variables1 | Frequency (n = 67) | Percentage |
|---|---|---|
Sex | ||
Female | 24 | 35.82% |
Male | 43 | 64.18% |
Age | ||
Mean (± Standard Deviation) | 69.66 (± 7.40) years | |
Presence of comorbidities | ||
Present | 50 | 74.63% |
Absent | 17 | 25.37% |
Types of comorbidities | ||
Hypertension | 38 | 56.72% |
Diabetes mellitus | 19 | 28.36% |
Chronic kidney disease | 9 | 13.43% |
Liver cirrhosis | 8 | 11.94% |
Medications used | ||
NSAID | 17 | 25.37% |
Anticoagulants | 14 | 20.90% |
Variables1 | Frequency (n = 67) | Percentage |
|---|---|---|
Clinical findings | ||
Abdominal pain | 13 | 19.40% |
Melena | 45 | 67.16% |
Hematemesis | 8 | 11.94% |
General body weakness | 36 | 53.73% |
Syncope | 5 | 7.46% |
Altered mental status | 4 | 5.97% |
Variables1 | Mean (± Standard Deviation) |
|---|---|
INR | 1.20 (± 0.14) |
BUN | 15.59 (± 10.99) |
Hemoglobin | 79.88 (± 21.73) |
Blood transfusion | 1.58 (± 1.78) |
Variables1 | Frequency (n = 67) | Percentage |
|---|---|---|
Endoscopic findings | ||
No active bleeding site | 15 | 22.39% |
Duodenal ulcer | 4 | 5.97% |
Duodenitis | 5 | 7.46% |
Gastric ulcer | 13 | 19.40% |
Gastritis | 32 | 47.76% |
Esophageal-gastric varices | 6 | 8.96% |
Mallory-Weiss tear | 2 | 2.99% |
Forrest grade | ||
Grade 1A | 1 | 1.49% |
Grade 1B | 1 | 1.49% |
Grade 2A | 3 | 4.48% |
Grade 2B | 6 | 8.96% |
Grade 2C | 9 | 13.43% |
Grade 3 | 47 | 70.15% |
Disposition | ||
Admitted to regular ward | 56 | 83.58% |
Admitted to Intensive Care Unit | 11 | 16.42% |
Mortality | ||
Survived | 59 | 88.06% |
Death | 8 | 11.94% |
Variables1 | Survived (n = 59) | Expired (n = 8) | p-values2,3 | ||
|---|---|---|---|---|---|
n | % | n | % | ||
Sex | |||||
Females | 22 | 37.29 | 2 | 25.00 | 0.496 |
Males | 37 | 62.71 | 6 | 75.00 | |
Age | 69.97 (± 7.18) | 67.38 (± 9.02) | 0.356 | ||
Comorbidities | |||||
Present | 43 | 72.88 | 7 | 87.50 | 0.373 |
Absent | 16 | 27.12 | 1 | 12.50 | |
Types of comorbidities | |||||
Hypertension | 33 | 55.93 | 5 | 62.50 | 0.725 |
Diabetes mellitus | 16 | 27.12 | 3 | 37.50 | 0.541 |
Chronic kidney disease | 7 | 11.86 | 2 | 25.00 | 0.307 |
Liver cirrhosis | 7 | 11.86 | 1 | 12.50 | 0.959 |
Medications used | |||||
NSAID | 16 | 27.12 | 1 | 12.50 | 0.373 |
Anticoagulants | 13 | 22.03 | 1 | 12.50 | 0.534 |
Clinical findings | |||||
Abdominal pain | 12 | 20.34 | 1 | 12.50 | 0.599 |
Melena | 40 | 67.80 | 5 | 62.50 | 0.765 |
Hematemesis | 7 | 11.86 | 1 | 12.50 | 0.959 |
General body weakness | 31 | 52.54 | 5 | 62.50 | 0.596 |
Syncope | 5 | 8.47 | - | - | 0.392 |
Altered mental status | 4 | 6.78 | - | - | 0.448 |
Laboratory findings | |||||
INR | 1.19 (± 0.12) | 1.27 (± 0.23) | 0.171 | ||
BUN | 14.65 (± 8.57) | 22.52 (± 21.64) | 0.057 | ||
Hemoglobin | 79.85 (± 22.29) | 80.13 (± 18.29) | 0.973 | ||
Blood transfusion | 1.54 (± 1.80) | 1.88 (± 1.64) | 0.623 | ||
Endoscopic findings | |||||
No active bleeding site | 13 | 22.03 | 2 | 25.00 | 0.850 |
Duodenal ulcer | 3 | 5.08 | 1 | 12.50 | 0.406 |
Duodenitis | 5 | 8.47 | - | - | 0.392 |
Gastric ulcer | 10 | 16.95 | 3 | 37.50 | 0.168 |
Gastritis | 28 | 47.46 | 4 | 50.00 | 0.893 |
Esophageal-gastric varices | 6 | 10.17 | - | - | 0.345 |
Mallory-Weiss tear | 2 | 3.39 | - | - | 0.597 |
Forrest grade | |||||
Grade 1A | 1 | 1.69 | - | - | 0.878 |
Grade 1B | 1 | 1.69 | - | - | |
Grade 2A | 2 | 3.39 | 1 | 12.50 | |
Grade 2B | 5 | 8.47 | 1 | 12.50 | |
Grade 2C | 8 | 13.56 | 1 | 12.50 | |
Grade 3 | 42 | 71.19 | 5 | 62.50 | |
Disposition | |||||
Admitted to regular ward | 55 | 93.22 | 1 | 12.50 | < 0.01** |
Admitted to ICU | 4 | 6.78 | 7 | 87.50 | |
Variables | Unadjusted OR / Coefficient | p-values1,2 | Adjusted OR / Coefficient | p-values1,2 |
|---|---|---|---|---|
Sex (Baseline: Males) | 0.561 | 0.501 | 0.396 | 0.413 |
Age | -0.052 | 0.355 | -0.041 | 0.323 |
Comorbidities (Baseline: None) | 2.605 | 0.388 | 2.287 | 0.287 |
Types of comorbidities (Baseline: None) | ||||
Hypertension | 1.313 | 0.726 | 1.189 | 0.601 |
Diabetes mellitus | 1.613 | 0.544 | 1.573 | 0.549 |
Chronic kidney disease | 2.476 | 0.319 | 1.475 | 0.269 |
Liver cirrhosis | 1.061 | 0.959 | 1.095 | 0.984 |
Medications used (Baseline: None) | ||||
NSAID | 0.384 | 0.388 | 0.425 | 0.445 |
Anticoagulants | 0.505 | 0.540 | 0.563 | 0.617 |
Clinical findings (Baseline: None) | ||||
Abdominal pain | 0.560 | 0.603 | 0.470 | 0.603 |
Melena | 0.792 | 0.765 | 0.619 | 0.633 |
Hematemesis | 1.061 | 0.959 | 1.212 | 0.894 |
General body weakness | 1.505 | 0.598 | 1.167 | 0.682 |
Syncope | - | - | - | - |
Altered mental status | - | - | - | - |
INR | 3.133 | 0.184 | 2.356 | 0.490 |
BUN | 0.049 | 0.084 | 0.028 | 0.092 |
Hemoglobin | 0.001 | 0.973 | 0.001 | 0.977 |
Blood transfusion | 0.100 | 0.618 | 0.099 | 0.654 |
Endoscopic findings | ||||
No active bleeding site | 1.179 | 0.850 | 1.130 | 0.708 |
Duodenal ulcer | 2.667 | 0.422 | 2.429 | 0.519 |
Duodenitis | - | - | - | - |
Gastric ulcer | 2.940 | 0.182 | 2.143 | 0.133 |
Gastritis | 1.107 | 0.893 | 1.253 | 0.385 |
Esophageal-gastric varices | - | - | - | - |
Mallory-Weiss tear | - | - | - | - |
Forrest grade (Baseline: Grade 3) | ||||
Grade 1A | - | - | - | - |
Grade 1B | - | - | - | - |
Grade 2A | 0.400 | 0.577 | 0.657 | 0.597 |
Grade 2B | 0.250 | 0.392 | 0.261 | 0.405 |
Grade 2C | 0.238 | 0.274 | 0.181 | 0.312 |
Disposition (Baseline: Regular ward) | 9.625 | < 0.01** | 9.382 | < 0.01** |
UGIB | Upper Gastrointestinal Bleeding |
EGD | Esophagogastroduodenoscopy |
ICU | Intensive Care Unit |
BUN | Blood Urea Nitrogen |
INR | International Normalize Ratio |
GI | Gastrointestinal |
NSAIDs | Nonsteroidal Anti-Inflammatory Drugs |
| [1] | Elkhatib FA. Acute upper gastrointestinal bleeding among early and late elderly patients. Dig Dis Sci. 2010 Oct; 55(10): 3007-9. |
| [2] | Thomopoulos KC, Vagenas KA, Vagianos CE, Margaritis VG, Blikas AP, Katsakoulis EC, et al. Changes in aetiology and clinical outcome of acute upper gastrointestinal bleeding during the last 15 years. Eur J Gastroenterol Hepatol 2004; 16: 177-82. |
| [3] | Ahmed, A., & Stanley, A. J. (2012). Acute upper gastrointestinal bleeding in the elderly. Drugs & Aging, 29(12), 933-940. |
| [4] | Alkhatib, A. A., Elkhatib, F. A., Alkhatib, A. A., Maldonado, A., Abubakr, S. M., & Adler, D. G. (2010). Acute upper gastrointestinal bleeding in elderly people: Presentations, endoscopic findings, and outcomes. Journal of the American Geriatrics Society, 58(1), 182-185. |
| [5] | Thongbai T, Thanapirom K, Ridtitid W, Rerknimitr R, Thungsuk R, Noophun P, Et Al. Factors Predicting Mortality Of Elderly Patients With Acute Upper Gastrointestinal Bleeding. Asian Biomedicine. 2016 Apr 1; 10(2): 115-22. |
| [6] |
Chandail, Vijantsingh, And Pranav Mahajan. “Etiological And Endoscopic Profile Of Middle Aged And Elderly Patients With Upper Gastrointestinal Bleeding In A Tertiary Care Hospital In North India: A Retrospective Analysis.” Journal Of Mid-Life Health, Vol. 8, No. 3, 2017, P. 137,
https://doi.org/10.4103/Jmh.Jmh_86_17 Accessed 1 Apr. 2022. |
| [7] | Bodh, V., Sharma, B., Kumar, R., & Sharma, R. (2021). Current Trends in Etiological Profile of Acute Upper Gastrointestinal Bleeding in Northern India: A Retrospective Analysis of 5-Year Endoscopic Data. Journal of Digestive Endoscopy, 12(01), 031-035. |
| [8] |
Abella, A. et al, A 5-year retrospective study on upper gastrointestinal bleeding based on esophago-gastro-duodenoscopy in Manila Central University Hospital. (2010-2014). 1(1),
https://registry.healthresearch.ph/index.php?view=research&cid=83558 |
| [9] |
Ching, M. C., Domingo, E., Gloria, V., Makalinao, A., & Limson, A. (1985, August 31). Upper gastrointestinal hemorrhage in the elderly. Philippine Journal of Internal Medicine.
https://registry.healthresearch.ph/index.php?view=research&cid=22289 |
| [10] | Lenti, M. V., Pasina, L., Cococcia, S., Cortesi, L., Miceli, E., Caccia Dominioni, C., Pisati, M., Mengoli, C., Perticone, F., Nobili, A., Di Sabatino, A., & Corazza, G. R. (2019b). Mortality rate and risk factors for gastrointestinal bleeding in elderly patients. European Journal of Internal Medicine, 61, 54-61. |
| [11] | Hossam, M., Abdel-Fattah, S., Elkholy, S. et al. Acute gastrointestinal bleeding in Egyptian elderly patients: real-life experience. Egypt Liver Journal 12, 33 (2022). |
| [12] | Hao, W., Liu, A., Zhu, H. et al. Risk factors and management of gastrointestinal bleeding in patients with or without antiplatelet and anticoagulation therapy: a multicenter real-world prospective study. BMC Gastroenterol 24, 155 (2024). |
| [13] | Charatcharoenwitthaya P, Pausawasdi N, Laosanguaneak N, Bubthamala J, Tanwandee T, Leelakusolvong S. Characteristics And Outcomes Of Acute Upper Gastrointestinal Bleeding After Therapeutic Endoscopy In The Elderly. World J Gastroenterol. 2011; 28; 17: 3724-32. |
| [14] | Minoru Tomizawa, Fuminobu Shinozaki, Rumiko Hasegawa, Yoshinori Shirai, Yasufumi Motoyoshi, Takao Sugiyama, Shigenori Yamamoto, And Naoki Ishige. Patient Characteristics With High Or Low Blood Urea Nitrogen In Upper Gastrointestinal Bleeding. World Journal Of Gastroenterology (2015) 21(24): 7500-7505. |
| [15] | Sato, K., & Lapus, J. (2018). Factors Predicting Mortality In Patients With Acute Upper Gastrointestinal Bleeding In Cardinal Santos Medical Center (P. 8) [Review Of Factors Predicting Mortality In Patients With Acute Upper Gastrointestinal Bleeding In Cardinal Santos Medical Center. |
| [16] | Anand, D. et al. (2014) ‘Clinical and endoscopic profile of patients with upper gastrointestinal bleeding at tertiary care center of North India’, Journal of Digestive Endoscopy, 05(04), pp. 139-143. |
| [17] | Elsebaey Ma, Elashry H, Elbedewy Ta, Elhadidy Aa, Esheba Ne, Ezat S, Et Al. Predictors Of In-Hospital Mortality In A Cohort Of Elderly Egyptian Patients With Acute Upper Gastrointestinal Bleeding.Medicine (Baltimore). 2018; 97: E0403. |
APA Style
Imperial, M. J. C., Lim-Teodoro, A., Sato, K. (2025). Clinical Profile of Filipino Elderly Patients with Upper Gastrointestinal Bleeding Admitted in a Tertiary Hospital: A Retrospective Cohort Study. International Journal of Gastroenterology, 9(1), 15-24. https://doi.org/10.11648/j.ijg.20250901.13
ACS Style
Imperial, M. J. C.; Lim-Teodoro, A.; Sato, K. Clinical Profile of Filipino Elderly Patients with Upper Gastrointestinal Bleeding Admitted in a Tertiary Hospital: A Retrospective Cohort Study. Int. J. Gastroenterol. 2025, 9(1), 15-24. doi: 10.11648/j.ijg.20250901.13
AMA Style
Imperial MJC, Lim-Teodoro A, Sato K. Clinical Profile of Filipino Elderly Patients with Upper Gastrointestinal Bleeding Admitted in a Tertiary Hospital: A Retrospective Cohort Study. Int J Gastroenterol. 2025;9(1):15-24. doi: 10.11648/j.ijg.20250901.13
@article{10.11648/j.ijg.20250901.13,
author = {Marie Jeramiah Concubierta Imperial and Adolf Lim-Teodoro and Kenji Sato},
title = {Clinical Profile of Filipino Elderly Patients with Upper Gastrointestinal Bleeding Admitted in a Tertiary Hospital: A Retrospective Cohort Study
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {1},
pages = {15-24},
doi = {10.11648/j.ijg.20250901.13},
url = {https://doi.org/10.11648/j.ijg.20250901.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250901.13},
abstract = {Background of the Study: Upper Gastrointestinal bleeding (UGIB) remains to be a significant clinical concern for geriatric patients due to their prolonged hospital stay and higher mortality and morbidity rates. The clinical profile of the geriatric patients are important aspects to consider, given that there is limited data in elderly population. Objective: The study is aimed to determine the clinical profile of elderly patients with UGIB admitted in a Tertiary Hospital from January 2024 to June 2024. Methods: This is a retrospective cohort study among elderly Filipino patients aged 60 years and above; admitted as UGIB and underwent esophagogastroduodenoscopy (EGD). Baseline Demographic, clinical presentation, laboratory results, endoscopic findings, prognosis and predictors of mortality were evaluated. Statistical analysis involved the application of Pearson’s chi-square, Fisher’s exact test, T-test and univariate and multivariate logistic regression analysis. Results: Among 102 admitted elderly patients with UGIB, 67 of them underwent EGD, thus were included in the study; 43 (64.18%) were male and 24 (35.82%) were female with the median age of 69.66 (±7.40) years. The prevalence rate of UGIB among elderly Filipino is 8.90%. 50 of those patients (74.63%) had comorbidities, the most common were: hypertension 38 (56.72%), diabetes mellitus 19 (28.36%) and chronic kidney diseases (13.43%). Patients presented mostly with melena (67.16%), generalized body weakness (53.73%) and 19.40% had abdominal pain. During endoscopy, (47.76%) was due to gastritis and gastric ulcer (19.40%). Mortality rate was higher in patients admitted at the ICU. No association was noted between the patients’ mortality and their sex, age, comorbidities, medications used, clinical findings, INR, BUN, hemoglobin, blood transfusion, and endoscopic findings. Conclusion: The present study reported that elderly patients with UGIB were male, with hypertension as the most common comorbidity. EGD findings showed gastritis as the most common cause of UGIB. Mortality rate is higher in patients admitted at the ICU. None of the variables showed significant differences in terms of predictors of mortality.
},
year = {2025}
}
TY - JOUR T1 - Clinical Profile of Filipino Elderly Patients with Upper Gastrointestinal Bleeding Admitted in a Tertiary Hospital: A Retrospective Cohort Study AU - Marie Jeramiah Concubierta Imperial AU - Adolf Lim-Teodoro AU - Kenji Sato Y1 - 2025/04/28 PY - 2025 N1 - https://doi.org/10.11648/j.ijg.20250901.13 DO - 10.11648/j.ijg.20250901.13 T2 - International Journal of Gastroenterology JF - International Journal of Gastroenterology JO - International Journal of Gastroenterology SP - 15 EP - 24 PB - Science Publishing Group SN - 2640-169X UR - https://doi.org/10.11648/j.ijg.20250901.13 AB - Background of the Study: Upper Gastrointestinal bleeding (UGIB) remains to be a significant clinical concern for geriatric patients due to their prolonged hospital stay and higher mortality and morbidity rates. The clinical profile of the geriatric patients are important aspects to consider, given that there is limited data in elderly population. Objective: The study is aimed to determine the clinical profile of elderly patients with UGIB admitted in a Tertiary Hospital from January 2024 to June 2024. Methods: This is a retrospective cohort study among elderly Filipino patients aged 60 years and above; admitted as UGIB and underwent esophagogastroduodenoscopy (EGD). Baseline Demographic, clinical presentation, laboratory results, endoscopic findings, prognosis and predictors of mortality were evaluated. Statistical analysis involved the application of Pearson’s chi-square, Fisher’s exact test, T-test and univariate and multivariate logistic regression analysis. Results: Among 102 admitted elderly patients with UGIB, 67 of them underwent EGD, thus were included in the study; 43 (64.18%) were male and 24 (35.82%) were female with the median age of 69.66 (±7.40) years. The prevalence rate of UGIB among elderly Filipino is 8.90%. 50 of those patients (74.63%) had comorbidities, the most common were: hypertension 38 (56.72%), diabetes mellitus 19 (28.36%) and chronic kidney diseases (13.43%). Patients presented mostly with melena (67.16%), generalized body weakness (53.73%) and 19.40% had abdominal pain. During endoscopy, (47.76%) was due to gastritis and gastric ulcer (19.40%). Mortality rate was higher in patients admitted at the ICU. No association was noted between the patients’ mortality and their sex, age, comorbidities, medications used, clinical findings, INR, BUN, hemoglobin, blood transfusion, and endoscopic findings. Conclusion: The present study reported that elderly patients with UGIB were male, with hypertension as the most common comorbidity. EGD findings showed gastritis as the most common cause of UGIB. Mortality rate is higher in patients admitted at the ICU. None of the variables showed significant differences in terms of predictors of mortality. VL - 9 IS - 1 ER -
Department of Internal Medicine, Quirino Memorial Medical Center, Quezon City, Philippines
Department of Internal Medicine, Quirino Memorial Medical Center, Quezon City, Philippines
Department of Internal Medicine, Cardinal Santos Medical Center, San Juan City, Philippines