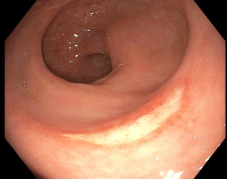
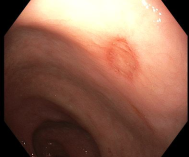
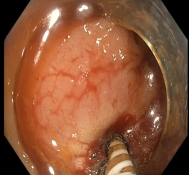
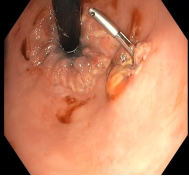
Background: Lower gastrointestinal (GI) bleeding is a significant cause of morbidity and mortality, with incidence rising with age. Stercoral ulcers, which are mucosal lesions in the colon or rectum, develop due to pressure from hardened or impacted fecal material. They primarily occur in elderly individuals with chronic constipation, dementia, or prolonged immobility, though they may also affect younger patients with psychiatric disorders. These ulcers can lead to bleeding or even perforation. While stercoral ulcers typically present with mild bleeding, massive GI haemorrhage is a rare but serious complication. Only a few reported cases describe stercoral ulcers with a visible vessel causing life-threatening lower GI bleeding. Case presentation: A 65-year-old woman with a history of hypertension, type 2 diabetes mellitus, and a recent ischemic stroke (resulting in left hemiparesis) on antiplatelet therapy presented with worsening chronic constipation and acute onset hematochezia. On examination, fecal impaction was suspected. Initial management with fluid resuscitation, blood transfusion, and manual fecal disimpaction was done. Subsequent sigmoidoscopy revealed multiple rectal ulcers of varying shapes and sizes, with one ulcer exhibiting a non-bleeding visible vessel. The lesion was successfully treated with endoscopic gold probe electrocoagulation, followed by haemostatic clip application to secure the vessel. The patient had no further bleeding episodes post-intervention. Conclusion: This case underscores the importance of proactive constipation management in elderly, bedridden patients, particularly those with multiple comorbidities and on antiplatelet therapy. Early recognition and intervention for stercoral ulcers are essential to prevent life-threatening complications such as massive gastrointestinal hemorrhage or perforation. Endoscopic therapy, including electrocoagulation and clipping, can be an effective approach for achieving hemostasis in such scenarios.
| Published in | International Journal of Gastroenterology (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijg.20250901.16 |
| Page(s) | 37-40 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Stercoral Ulcer, Massive Lower GI Bleed, Constipation
LGIB | Lower Gastrointestinal Bleeding |
GI | Gastrointestinal |
| [1] | Grinvalsky HT, Bowerman CI. Stercoraceous ulcers of the colon: relatively neglected medical and surgical problem. J Am Med Assoc. 1959 Dec 5; 171: 1941–6. |
| [2] | Ünal E, Onur MR, Balcı S, Görmez A, Akpınar E, Böge M. Stercoral colitis: diagnostic value of CT findings. Diagn Interv Radiol. 2017 Jan; 23(1): 5–9. |
| [3] | Knigge KL, Katon RM. Massive hematochezia from a visible vessel within a stercoral ulcer: effective endoscopic therapy. Gastrointest Endosc. 1997 Oct; 46(4): 369–70. |
| [4] | Chait MM. Lower gastrointestinal bleeding in the elderly. World J Gastrointest Endosc. 2010 May 16; 2(5): 147–54. |
| [5] | Adegboyega T, Rivadeneira D. Lower GI Bleeding: An Update on Incidences and Causes. Clin Colon Rectal Surg. 2020 Jan; 33(1): 28–34. |
| [6] | Ghassemi KA, Jensen DM. Lower GI Bleeding: Epidemiology and Management. Curr Gastroenterol Rep. 2013 Jul; 15(7): |
| [7] | Berry J. Dilatation and rupture of the sigmoid flexure. Br Med J. 1984; 1: 301–2. |
| [8] | Heffernan C, Pachter HL, Megibow AJ, Macari M. Stercoral colitis leading to fatal peritonitis: CT findings. AJR Am J Roentgenol. 2005 Apr; 184(4): 1189–93. |
| [9] | Hotiana MM, Amaryl R, Athar MN, Hussain SN, Altaf M. Stercoral Ulcer. An Uncommon Cause of Lower GI Bleeding: Case Report and Review of Literature: 480. Official journal of the American College of Gastroenterology | ACG. 2005 Sep; 100: S182. |
| [10] | Hassranah S, Maharajh S, Solomon S, Naraynsingh V. Massive Rectal Hemorrhage From a Stercoral Ulcer. Cureus. 14(7): e26963. |
| [11] | Huang CC, Wang IF, Chiu HH. Lower gastrointestinal bleeding caused by stercoral ulcer. CMAJ. 2011 Feb 8; 183(2): E134–E134. |
| [12] | Matsushita M, Hajiro K, Takakuwa H, Nishio A, Tominaga M. Bleeding stercoral ulcer with visible vessels: effective endoscopic injection therapy without electrocoagulation. Gastrointest Endosc. 1998 Nov; 48(5): 559. |
APA Style
Deshidi, S., Mahajan, G., Kamisetty, V., Kolla, S., Gongati, V., et al. (2025). Stercoral Ulcers with Visible Vessel Presenting as Massive Lower Gastrointestinal Bleeding. International Journal of Gastroenterology, 9(1), 37-40. https://doi.org/10.11648/j.ijg.20250901.16
ACS Style
Deshidi, S.; Mahajan, G.; Kamisetty, V.; Kolla, S.; Gongati, V., et al. Stercoral Ulcers with Visible Vessel Presenting as Massive Lower Gastrointestinal Bleeding. Int. J. Gastroenterol. 2025, 9(1), 37-40. doi: 10.11648/j.ijg.20250901.16
AMA Style
Deshidi S, Mahajan G, Kamisetty V, Kolla S, Gongati V, et al. Stercoral Ulcers with Visible Vessel Presenting as Massive Lower Gastrointestinal Bleeding. Int J Gastroenterol. 2025;9(1):37-40. doi: 10.11648/j.ijg.20250901.16
@article{10.11648/j.ijg.20250901.16,
author = {Srinu Deshidi and Gaurav Mahajan and Vishwanath Kamisetty and Spoorthi Kolla and Venu Gongati and Gongala Harshvardhan Reddy and Bhaskar Kante and Sreekanth Appasani},
title = {Stercoral Ulcers with Visible Vessel Presenting as Massive Lower Gastrointestinal Bleeding
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {1},
pages = {37-40},
doi = {10.11648/j.ijg.20250901.16},
url = {https://doi.org/10.11648/j.ijg.20250901.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250901.16},
abstract = {Background: Lower gastrointestinal (GI) bleeding is a significant cause of morbidity and mortality, with incidence rising with age. Stercoral ulcers, which are mucosal lesions in the colon or rectum, develop due to pressure from hardened or impacted fecal material. They primarily occur in elderly individuals with chronic constipation, dementia, or prolonged immobility, though they may also affect younger patients with psychiatric disorders. These ulcers can lead to bleeding or even perforation. While stercoral ulcers typically present with mild bleeding, massive GI haemorrhage is a rare but serious complication. Only a few reported cases describe stercoral ulcers with a visible vessel causing life-threatening lower GI bleeding. Case presentation: A 65-year-old woman with a history of hypertension, type 2 diabetes mellitus, and a recent ischemic stroke (resulting in left hemiparesis) on antiplatelet therapy presented with worsening chronic constipation and acute onset hematochezia. On examination, fecal impaction was suspected. Initial management with fluid resuscitation, blood transfusion, and manual fecal disimpaction was done. Subsequent sigmoidoscopy revealed multiple rectal ulcers of varying shapes and sizes, with one ulcer exhibiting a non-bleeding visible vessel. The lesion was successfully treated with endoscopic gold probe electrocoagulation, followed by haemostatic clip application to secure the vessel. The patient had no further bleeding episodes post-intervention. Conclusion: This case underscores the importance of proactive constipation management in elderly, bedridden patients, particularly those with multiple comorbidities and on antiplatelet therapy. Early recognition and intervention for stercoral ulcers are essential to prevent life-threatening complications such as massive gastrointestinal hemorrhage or perforation. Endoscopic therapy, including electrocoagulation and clipping, can be an effective approach for achieving hemostasis in such scenarios.
},
year = {2025}
}
TY - JOUR T1 - Stercoral Ulcers with Visible Vessel Presenting as Massive Lower Gastrointestinal Bleeding AU - Srinu Deshidi AU - Gaurav Mahajan AU - Vishwanath Kamisetty AU - Spoorthi Kolla AU - Venu Gongati AU - Gongala Harshvardhan Reddy AU - Bhaskar Kante AU - Sreekanth Appasani Y1 - 2025/05/24 PY - 2025 N1 - https://doi.org/10.11648/j.ijg.20250901.16 DO - 10.11648/j.ijg.20250901.16 T2 - International Journal of Gastroenterology JF - International Journal of Gastroenterology JO - International Journal of Gastroenterology SP - 37 EP - 40 PB - Science Publishing Group SN - 2640-169X UR - https://doi.org/10.11648/j.ijg.20250901.16 AB - Background: Lower gastrointestinal (GI) bleeding is a significant cause of morbidity and mortality, with incidence rising with age. Stercoral ulcers, which are mucosal lesions in the colon or rectum, develop due to pressure from hardened or impacted fecal material. They primarily occur in elderly individuals with chronic constipation, dementia, or prolonged immobility, though they may also affect younger patients with psychiatric disorders. These ulcers can lead to bleeding or even perforation. While stercoral ulcers typically present with mild bleeding, massive GI haemorrhage is a rare but serious complication. Only a few reported cases describe stercoral ulcers with a visible vessel causing life-threatening lower GI bleeding. Case presentation: A 65-year-old woman with a history of hypertension, type 2 diabetes mellitus, and a recent ischemic stroke (resulting in left hemiparesis) on antiplatelet therapy presented with worsening chronic constipation and acute onset hematochezia. On examination, fecal impaction was suspected. Initial management with fluid resuscitation, blood transfusion, and manual fecal disimpaction was done. Subsequent sigmoidoscopy revealed multiple rectal ulcers of varying shapes and sizes, with one ulcer exhibiting a non-bleeding visible vessel. The lesion was successfully treated with endoscopic gold probe electrocoagulation, followed by haemostatic clip application to secure the vessel. The patient had no further bleeding episodes post-intervention. Conclusion: This case underscores the importance of proactive constipation management in elderly, bedridden patients, particularly those with multiple comorbidities and on antiplatelet therapy. Early recognition and intervention for stercoral ulcers are essential to prevent life-threatening complications such as massive gastrointestinal hemorrhage or perforation. Endoscopic therapy, including electrocoagulation and clipping, can be an effective approach for achieving hemostasis in such scenarios. VL - 9 IS - 1 ER -
Krishna Institute of Medical Sciences, Hyderabad, India
Indian Naval Hospital Ship Asvini, Mumbai, India
Krishna Institute of Medical Sciences, Hyderabad, India
Krishna Institute of Medical Sciences, Hyderabad, India
Krishna Institute of Medical Sciences, Hyderabad, India
Krishna Institute of Medical Sciences, Hyderabad, India
Krishna Institute of Medical Sciences, Hyderabad, India
Krishna Institute of Medical Sciences, Hyderabad, India