Abstract
Background: Inflammatory bowel disease (IBD) is associated with frequent hospitalizations, significant disability and impairment of quality of life. This can affect the physical, mental and overall wellbeing of not just the patients, but also the people caring for them. The aim of this study was to estimate the prevalence of burden among caregivers of young IBD patients, assess their work productivity impairment and identify the factors affecting caregiver burden. Methods: Design: This was a cross-sectional study conducted over a 16 month period at a tertiary care centre in north Kerala. Participants: 78 caregivers corresponding to 78 consecutive young IBD patients (aged 10- 24 years) were included. Two sets of questionnaires, the Zarit Burden Interview and the Work Productivity and Activity Impairment questionnaires tailored to suit IBD were used to assess burden and work productivity losses respectively. The study was approved by the institutional ethical committee. Results: A total of 78 caregivers, corresponding to 78 young IBD patients (aged 10- 24 years) were included in the study. 61 patients had Crohn’s disease and 17 patients had ulcerative colitis. Of the total number of caregivers, 47 caregivers (60.3%) experienced clinically significant caregiver burden. The mean ZBI score was 21.74± 10.3. The mean percentage work time missed (absenteeism) was 22.39%, the mean percentage impairment while working (presenteeism) was 40.0% and the mean percentage overall work impairment (loss of productivity) was 48.62%. Disease activity at the time of diagnosis (p=0.008 for Crohn’s p=0.002 for ulcerative colitis), absenteeism, presenteeism, work productivity loss and percentage activity impairment were significantly associated with caregiver burden Conclusion: Caregivers of young IBD patients experience significant burden and work productivity loss and this needs urgent attention to improve overall patient management.
Keywords
Caregiver Burden, Inflammatory Bowel Disease, Crohn’s Disease, Ulcerative Colitis, Work Productivity and Activity Impairment, Absenteeism, Presenteeism
1. Introduction
Inflammatory bowel disease (IBD) is a chronic disease that requires long term treatment. It includes 3 categories- Crohn’s disease (CD), Ulcerative Colitis (UC) and indeterminate type.
In adults, CD occurred at a younger age compared to UC, whereas the trend is opposite in children
| [1] | Philip M, Augustine P, Thomas V, Ramesh GN, Vinayakumar KR, Ramachandran TM, et al. Multi-center prospective survey of inflammatory bowel diseases in Kerala: More than 2000 cases. Indian J Gastroenterol. 2017 Nov 1; 36(6): 459-67. |
[1]
.
WHO defines “young people” as those aged between 10-24 years
. In India, most of the patients in this age group are still in their student life with no independent means of livelihood. When IBD affects this age group, they are highly dependent on their immediate family.
IBD has a highly unpredictable course. A study
| [3] | Lönnfors S, Vermeire S, Greco M, Hommes D, Bell C, Avedano L. IBD and health-related quality of life — Discovering the true impact. Journal of Crohn’s and Colitis. 2014 Oct; 8(10): 1281-6. |
[3]
published in 2014, showed that 22% of IBD patients, had periodic flares and during such flares, many required hospital admissions and had disabling GI bleeding.
The caregiver has to manage many responsibilities. They are expected to manage the frequent hospital visits, medication charges, hospital bills, communication with school or college (regarding frequent restroom visits, school absence in case of flares, poor scholastic performance due to disease activity and so on) and communication with the patient itself. This is in addition to the caregivers’ issues at workplace and in other relationships. Caregiver burden sums up these physical, mental, emotional, psychological, social and financial stresses associated with caring for a patient with IBD. A study by Aria Zand et al,
| [4] | Zand A, Kim BJ, van Deen WK, Stokes Z, Platt A, O’Hara S, et al. The effects of inflammatory bowel disease on caregivers: significant burden and loss of productivity. BMC Health Services Research. 2020 Jun 18; 20(1): 556. |
[4]
showed that 39% of caregivers experienced caregiver burden.
A review article published in 2018
| [5] | Shukla R, Thakur E, Bradford A, Hou JK. Caregiver Burden in Adults with Inflammatory Bowel Disease. Clin Gastroenterol Hepatol. 2018 Jan; 16(1): 7-15. |
[5]
describes psychological distress, decrease in physical health, sleep disturbance, negative changes in lifestyle, social isolation and decreased work productivity in caregivers of adult IBD patients. There are a few other studies in this area
| [6] | Guilfoyle SM, Denson LA, Baldassano RN, Hommel KA. Paediatric parenting stress in inflammatory bowel disease: application of the Pediatric Inventory for Parents. Child Care Health Dev. 2012 Mar; 38(2): 273-9. |
| [7] | Greenley RN, Cunningham C. Parent quality of life in the context of pediatric inflammatory bowel disease. J Pediatr Psychol. 2009 Mar; 34(2): 129-36. |
| [8] | Burke PM, Neigut D, Kocoshis S, Chandra R, Sauer J. Correlates of depression in new onset pediatric inflammatory bowel disease. Child Psychiatry Hum Dev. 1994; 24(4): 275-83. |
| [9] | Kahn SA, Lin CW, Ozbay B, Wang A, Chao J, Skup M. Indirect Costs and Family Burden of Pediatric Crohn’s Disease in the United States. Inflammatory Bowel Diseases. 2017 Dec 1; 23(12): 2089-96. |
| [10] | Klomberg RCW, Aardoom MA, Kemos P, Rizopoulos D, Ruemmele FM, Croft NM, et al. High Impact of Pediatric Inflammatory Bowel Disease on Caregivers’ Work Productivity and Daily Activities: An International Prospective Study. J Pediatr. 2022 Jul; 246: 95-102. e4. |
[6-10].
Guilfoyle et al
| [6] | Guilfoyle SM, Denson LA, Baldassano RN, Hommel KA. Paediatric parenting stress in inflammatory bowel disease: application of the Pediatric Inventory for Parents. Child Care Health Dev. 2012 Mar; 38(2): 273-9. |
[6]
, studied the psychosocial functioning of caregivers of adolescents managing IBD. They found a positive association between parenting stress and IBD disease severity. Caregiver age was found to be negatively associated with parenting stress. The study also compared the rate of parenting stress in caregivers of adolescent IBD patients with those in other chronic pediatric diseases and type I diabetes and concluded that parenting stress in the IBD sample was same as that in type 1 diabetes, but was much lower to rates identified in other pediatric chronic conditions like cancer, obesity, sickle cell disease.
Greenley et al,
| [7] | Greenley RN, Cunningham C. Parent quality of life in the context of pediatric inflammatory bowel disease. J Pediatr Psychol. 2009 Mar; 34(2): 129-36. |
[7]
studied forty nine patients with IBD (aged 10-18) and a parent each and they were asked to complete measures of demographics, parent quality of life, and youth quality of life. A greater activity of disease corresponded with lower quality of life in the parent in mental health and physical health domains. Higher youth quality of life was associated with higher parent quality of life in the mental health domain only.
Burke et al documented a lifetime depression rate of 51% in mothers of youth with IBD. Moreover, 10% of their sample was depressed at the time of the study
| [8] | Burke PM, Neigut D, Kocoshis S, Chandra R, Sauer J. Correlates of depression in new onset pediatric inflammatory bowel disease. Child Psychiatry Hum Dev. 1994; 24(4): 275-83. |
[8]
.
Kahn et al studied work loss and productivity costs among caregivers of pediatric CD patients and concluded that caregivers of pediatric CD patients had significantly higher loss in productivity costs compared with controls
| [9] | Kahn SA, Lin CW, Ozbay B, Wang A, Chao J, Skup M. Indirect Costs and Family Burden of Pediatric Crohn’s Disease in the United States. Inflammatory Bowel Diseases. 2017 Dec 1; 23(12): 2089-96. |
[9]
.
A study by Klomberg et al,
| [10] | Klomberg RCW, Aardoom MA, Kemos P, Rizopoulos D, Ruemmele FM, Croft NM, et al. High Impact of Pediatric Inflammatory Bowel Disease on Caregivers’ Work Productivity and Daily Activities: An International Prospective Study. J Pediatr. 2022 Jul; 246: 95-102. e4. |
[10]
found a mean work productivity loss of 44.6% and the adjusted mean activity impairment of 34.3% among caregivers of pediatric IBD patients. Work productivity loss and activity impairment significantly decreased over time and was found to be associated with activity of the disease. But it was not associated with the type of IBD child’s age. In this study, HRQOL was not seen to be related to disease duration or IBD type, but with the child’s age at diagnosis and disease activity. They also found an independent association between caregivers’ HRQOL and work productivity loss. Similarly, caregivers’ HRQOL was independently associated with activity impairment.
A recent multicentre trial
| [11] | Banerjee R, Pal P, Hilmi I, Raghunathan N, Rahman M, Limsrivillai J, Kamani L, Ghoshal UC, Aye TT, Joshi N, Alavinejad P, Peddi K, Patel R, Godbole S, Reddy DN. Primary caregiver burden and undiagnosed mental health illness in out-patients with inflammatory bowel disease-A multicentric prospective survey from the IBD Emerging Nations' Consortium. Indian J Gastroenterol. 2024 Dec; 43(6): 1156-1167. https://doi.org/10.1007/s12664-024-01617-y Epub 2024 Jul 18. |
[11]
, burden and mental illness among caregivers were explored. In this study, moderate to severe depression was found in 34% and anxiety was found in 24% of the bystanders.
The aim of our study was to assess the burden on the caregivers of young IBD patients and identify its predictors.
The study also aimed to assess the loss of work productivity in these caregivers and relationship between caregiver burden and work productivity loss.
2. Methods
2.1. Study Design and Setting
The study was a cross sectional study conducted in the Department of Medical Gastroenterology, Government Medical College, Kozhikode from January 2023 to April 2024.
2.2. Inclusion Criteria
Caregivers of known IBD patients with patient age- 10-24 years.
Caregivers with age more than 18 years and less than 75 years.
2.3. Exclusion Criteria
Caregivers younger than 18 years or older than 75 years.
Caregivers with other severe chronic illnesses- CKD, CLD, heart failure, respiratory failure, dementia and psychiatric illnesses (with onset before diagnosis of IBD) were excluded.
2.4. Materials and Questionnaires
All consecutive patients and caregivers who met the inclusion criteria were included in the study. A proforma was drafted to obtain the following -
1) Patient’s biodata- name, age, gender, address, contact number
2) Disease profile and severity- Montreal classification for CD and UC, CDAI, TLW
3) Medication adherence
The caregiver interviews were conducted using the following questionnaires and proformas:
a) Data on basic demographics
b) The Zarit Burden Interview Score (ZBI) [
12], a set of 22 questions that determine a caregiver’s burden- categorizes caregiver burden as following levels:
1) Little or no burden (score 0-21)
2) Mild to moderate burden (score 21-40)
3) Moderate to severe burden (score 41-60)
4) Severe burden (score≥61)
Total score range= 0-88.
Burden of level 2 or greater was considered clinically significant
c) The Work Productivity and Activity Impairment Questionnaire for caregivers (WPAI-CG),
| [13] | Mc R, As Z, Em D. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics [Internet]. 1993 Nov [cited 2022 Nov 8]; 4(5). Available from: https://pubmed.ncbi.nlm.nih.gov/10146874/ |
[13]
is a set of 6 questions. Those working for pay were required to answer all the 6 questions while those who were unemployed needed to answer only questions 1 and 6. Questions 5 and 6 were scored from 0 to 10.
Four parameters were derived using the answers of the questionnaire.
a) Absenteeism (percentage work time missed), b) Presenteeism (percentage impairment while working), c) work productivity loss- percentage overall work impairment, d) percentage activity impairment.
2.5. Statistical Analysis
Descriptive statistics were provided for the categorical variables. The results of the questionnaire were described as frequencies as well as total score. Mean, median and mode were calculated for the numerical variables. The relationship between variables were assessed using Chi square test, Pearson correlation and binary logistic regression models. SPSS software was used for data analysis.
2.6. Institutional Research Board Approval
The study has been approved by the institutional research and ethical committee: protocol number GMCKKD/RP2023/IEC/16.
3. Results
A total of 78 IBD patients in the specified age groups and one caregiver each were included in the study. Out of these, 61 patients had Crohn’s disease and 17 had ulcerative colitis - all were diagnosed clinically, endoscopically and histologically. All the caregivers in the study were family caregivers.
3.1. Demographic
Majority of the patients and caregivers were from the northern districts of Keral a (a southern state in India), where the study centre itself is located (42% from Malappuram, 29% from Kozhikode and 12.8% from Wynad).
3.1.1. Age and Gender
Most of the patients were in the 16-20 years age group and the mean patient age was 17.6 years. Most of the Crohn’s disease patients were in the 16-20 years age group (38%) while 53% of the ulcerative colitis patients were older (21-24 years). 52.5% of the patients in the study were males while 47.5% were females. A similar trend was seen in the Crohn’s patients with majority being males (57.4%) while in ulcerative colitis cases, majority of the patients were females (62.5%).
Most of the caregivers in the study were in the 31-40 years age group (42.3%). In ulcerative colitis, the age of the caregivers was older. 57% of the caregivers were females and 42% were males. 57% were mothers of the patients, 33% were fathers, 4% siblings, 5% spouse.
3.1.2. Caregiver Education and Employment Status
All the caregivers were literate. 69% had completed higher secondary education, 17% had only attended primary school, 11% were graduates and 3% were post graduates.
47% of the caregivers were working at the time of the interview, while 53% were not employed. Of the working population, 60% were daily wage workers while 40% had white collar jobs.
3.2. Patient Disease Characteristics
13 patients (16.7%) had a disease duration of less than or equal to a year, 48 patients (61.5%) had disease duration of 1-5 years, 15 (19.2%) had disease duration of 5-10 years and 2 patients (2.6%) had disease duration of 10 or more years.
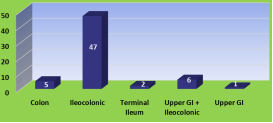
The disease location in patients with Crohn’s disease in our study is given in
Figure 1. Of the ulcerative colitis patients, 9 had pancolitis (52.9%), 2 each (11.8%) had proctosigmoiditis and left sided colitis while 4 had extensive colitis.
Figure 1. Disease location in patients - Crohn’s disease.
The numbers denote the number of patients with the particular disease location. 47(77%) had ileocolonic disease, 6(9.8%) had upper GI involvement with ileocolonic disease, 5(8.2%) had pure colitis, 2 (3.3%) had isolated terminal ileal disease while 1 had involvement of upper GI tract alone.
Of the Crohn’s disease patients, 74% had non stricturing, non-penetrating disease, 20% had stricturing disease behaviour and 6% had penetrating disease. 54% of the Crohn’s patients had disease involving perianal area.
At the onset of their disease, 47.5% of the Crohn’s disease patients included in the study had a CDAI score between 221 -450, 31% had CDAI score 1-150, 13% had 151-220 and 8.25 had CDAI score >450.
Overall, 53% of the study patients were in remission at the time of the interview while 47% had active disease. Regarding Crohn’s patients, 46% were in remission at the time of study while 54% had active disease (In ulcerative colitis group, 76% were in remission while 24% had active disease).
24% of the study patients had taken antituberculosis treatment previously.
14% of the study patients had undergone surgery previously for luminal or perianal disease or its complications.
Table 1 summarises the patients on biologicals and small molecules.
Table 1. Patients on Biologicals/small molecules-Crohn’s disease (CD) and Ulcerative colitis (UC).
| Crohn’s disease | Ulcerative Colitis |
No | 24 (39.3%) | 11 (64.7%) |
Infliximab | 29 (47.5%) | 4 (23.5%) |
Adalimumab | 8 (13.1%) | |
Tofacitinib | | 2 (11.8%) |
Total | 61 (100%) | 17 (100%) |
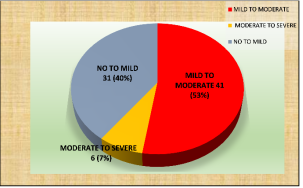
3.3. ZBI Burden
The burden of caregivers as per ZBI score is given in
Figure 2.
Figure 2. Degree of burden according to ZBI scoring. 53% had mild to moderate burden (ZBI score 21-40) and 7% had moderate to severe burden (ZBI score 41-60).
The mean ZBI burden was 21.74 (22.74 for Crohn’s caregivers and 18.18 for UC caregivers).
Table 2. Total Zarit Burden Interview (ZBI) score.
Mean | 21.74 |
Median | 22.00 |
Mode | 24 |
Std. Deviation | 10.365 |
Range | 50 |
Minimum | 0 |
Maximum | 50 |
ZBI questionnaire responses are summarised in the table provided in the supplementary data.
3.4. Possible Factors Affecting Burden
Among the caregivers, 29 out of 45 (64%) mothers experienced burden, 16 out of 26 fathers (61.5%) had burden and so did 50% of spouses (p=0.109).
The study found no significant association between caregiver age group and burden (p=0.551).
17 out of the 33 male caregivers (51.5%) and 30 out of the 45 females (66%) experienced significant burden. (p=0.177).
9 out of 13(69%) caregivers with primary school education, 62.9% (34 out of 54) with higher secondary education, 44% of graduates and none of the post graduates experienced clinically significant burden. This inverse relationship with higher education level was however not statistically significant. (p=0.156).
23 out of 37(62.1%) of the caregivers who were not working experienced burden while 58.5% of those who were employed experienced burden. (p=0.74).
Among Crohn’s patients, 63% caregivers of patients with ileocolonic disease experienced burden and so did 66%, 60%, 50% and 0% respectively of those with ileocolonic with upper GI involvement, isolated colitis, terminal ileal disease alone and those with upper GI involvement alone (p=0.70).
In ulcerative colitis, 55% of caregivers of patients with pancolitis, and 50% each of those with extensive colitis while none with proctosigmoiditis experienced burden.
20 out of 33(60%) Crohn’s disease patients with perianal involvement had caregivers who experienced burden while 18 of 28(64.2%) of those without perianal disease had burden (p=0.97).
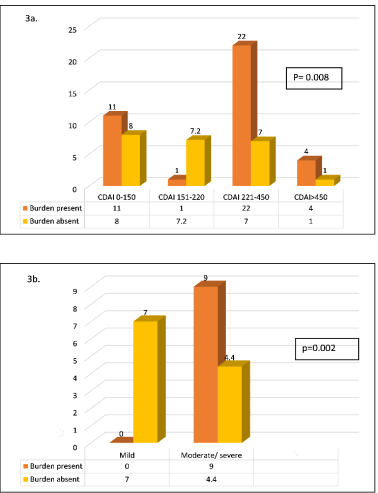
The initial disease activity of the corresponding patient in both Crohn’s disease and ulcerative colitis was significantly associated with caregiver burden (
Figure 3).
Figure 3. Initial disease activity and burden; 3a-Crohn’s disease, 3b- Ulcerative colitis CDAI: Crohn’s Disease Activity Index.
Caregivers of 24 out of 37 patients (64.8%) with active disease at the time of interview experienced burden compared to those of 23 out of 41 patients (56%) in remission- p=0.427.
46% of caregivers of patients with disease duration 1 year or less had burden and so did 58.3%, 73% and 100% of those with disease duration of 1-5 years, 5-10 years and > 10 years respectively (P=0.23).
44% patients in the study were not on biologicals or small molecules of which 54.2% experienced clinically significant burden. 63.6% of the caregivers of 33 patients on Infliximab, 75% of those on Adalimumab experienced burden and so did caregiver of 1 out of the 2 ulcerative colitis pattients on Tofacitinib.
3.5. WPAI Scores
The effect on the work productivity of caregivers assessed using the WPAI questionnaire is summarised in
Table 3.Table 3. Work Productivity and Activity Index (WPAI) scores.
| Hours of work missed in last 7 days | Hours of work missed due to other reasons | Mean hours of work in the past week | Percentage Work Time Missed (Absenteeism) | Percent Impairment while working (presenteeism) | Percent Overall Work impairment | Percent Activity impair-ment |
Mean | 12.13 | 5.80 | 48.23 | 22.39 | 40.00 | 48.62 | 38.59 |
Median | 8.00 | 6.00 | 49.00 | 15.14 | 40.00 | 50.50 | 40.00 |
Standard. Deviation | 15.34 | 5.79 | 20.71 | 27.43 | 30.17 | 32.12 | 31.67 |
Minimum | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Maximum | 84 | 24 | 80 | 100 | 100 | 862.0 | 100 |
Comparison between characteristics of caregivers with and without burden are summarised in the table given in supplementary material.
4. Discussion
The importance of caregiver burden in case of several chronic diseases has long been recognised. The small study by Akobeng et al,
| [14] | Akobeng AK, Miller V, Firth D, Suresh-Babu MV, Mir P, Thomas AG. Quality of life of parents and siblings of children with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 1999 Apr; 28(4): S40-42. |
[14]
studied 20 parents and 7 siblings of children with IBD and found that 65% parents were worried about their child’s future prospects and 55% were concerned about the problems likely at school.
Our study included 78 primary caregivers of IBD patients who were in the WHO defined “young people” age group (aged 10-24 years). There was a disproportionate recruitment of Crohn’s disease patients as compared to ulcerative colitis (n=61 for Crohn’s vs n= 17 for ulcerative colitis) in our study. This is a reflection of the epidemiology due to the specific age group of the patients included in the study. Western data reports the mean age at diagnosis of CD to be a decade earlier than UC
| [15] | Loftus EV, Sandborn WJ. Epidemiology of inflammatory bowel disease. Gastroenterol Clin North Am. 2002 Mar; 31(1): 1-20. |
| [16] | Makharia GK, Ramakrishna BS, Abraham P, Choudhuri G, Misra SP, Ahuja V, et al. Survey of inflammatory bowel diseases in India. Indian J Gastroenterol. 2012 Dec; 31(6): 299-306. |
| [17] | Wang YF, Zhang H, Ouyang Q. Clinical manifestations of inflammatory bowel disease: East and West differences. J Dig Dis. 2007 Aug; 8(3): 121-7. |
[15-17]
.
Most of the Crohn’s disease patients in our study had ileocolonic disease (77%). 54% had perianal disease, a much higher prevalence compared to population-based studies. This again maybe explained by the age group of patients included in the study (as perianal disease is known to be more common in younger patients). Another reason maybe the selection bias due to referral of complicated and severe cases. 60% of the Crohn’s disease patients in our study were on biologicals- all of them on anti TNF (n=29 on Infliximab and n=8 on Adalimumab). The biologicals were being given free of cost under the government health insurance scheme.
Among the 17 UC patients, 9 (53%) had pancolitis. 4 patients were on Infliximab and 2 were on Tofacitinib.
All the caregivers were family caregivers, 57.7% were females. The mean caregiver age was 41.46. Majority were mothers (57.6%). Others were patients’ father (n=26, 33.3%), siblings (n=3, 3.8%) or spouse (n=4). 47% of the caregivers were employed and of these, 60% were daily wage workers. Majority of the caregivers had a higher secondary level education. Most families were below the poverty line. The monthly income ranged from Rs 900 to Rs 80,000.
Each caregiver was subjected to a one-time interview based on the Zarit Burden Interview (ZBI) questionnaire. Originally designed
| [12] | Bédard M, Molloy DW, Squire L, Dubois S, Lever JA, O’Donnell M. The Zarit Burden Interview: a new short version and screening version. Gerontologist. 2001 Oct; 41(5): 652-7. |
| [18] | Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980 Dec; 20(6): 649-55. |
[12, 18]
to assess caregiver burden in other chronic illnesses, many studies have used it in IBD
. 52% of the caregivers in our study experienced mild-moderate burden (ZBI score ≥21), 6 caregivers had moderate- severe burden (score 41-60). Both these categories indicate clinically significant burden. So, 60% of our caregivers had clinically relevant caregiver burden. The mean ZBI score was 21.74 with a standard deviation of 10.36. Study by Aria Zand,
| [4] | Zand A, Kim BJ, van Deen WK, Stokes Z, Platt A, O’Hara S, et al. The effects of inflammatory bowel disease on caregivers: significant burden and loss of productivity. BMC Health Services Research. 2020 Jun 18; 20(1): 556. |
[4]
found caregiver burden in 39% of caregivers while in the Parekh study, it was 43.8% (mean ZBI score was 19.9±11.07). Our study shows a much higher burden in IBD caregivers of young patients. Moreover, 43% of the caregivers “were stressed about caregiving”, 83% were afraid of “what the future of their patient would be”, 51% felt that they were “losing control over life” after the diagnosis and 62% caregivers “felt burdened” in one way or the other.
Caregivers of patients who were still in school or college, also raised a major concern regarding the child’s future education and career (77%). The frequent hospitalisations and disease flares led to significant school absenteeism and many caregivers felt it would be helpful if teachers and school authorities were more informed regarding the nature of the disease. Another major area of concern was the financial burden (74% of caregivers felt that they did not have enough money to care for their patient).
Other means to assess caregiver burden include the questionnaire by Cliff and MacDonagh
, IBD specific 14 items questionnaire by Vergara et al
| [21] | Assessing the quality of life of household members of patients with inflammatory bowel disease: development and validation of a specific questionnaire - PubMed [Internet]. [cited 2024 Jul 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/12094861/ |
[21]
and also the Paediatric Inventory for Parents (PIP)
| [22] | Gray WN, Graef DM, Schuman SS, Janicke DM, Hommel KA. Parenting Stress in Pediatric IBD: Relations with Child Psychopathology, Family Functioning, and Disease Severity. Journal of Developmental & Behavioral Pediatrics. 2013 May; 34(4): 237-44. |
[22]
.
The mean percentage overall work impairment (Work productivity loss) using WPAI questionnaire in our study was 48.62%. In the study by Klomberg et al,
| [10] | Klomberg RCW, Aardoom MA, Kemos P, Rizopoulos D, Ruemmele FM, Croft NM, et al. High Impact of Pediatric Inflammatory Bowel Disease on Caregivers’ Work Productivity and Daily Activities: An International Prospective Study. J Pediatr. 2022 Jul; 246: 95-102. e4. |
[10]
the average time worked in the previous week by employed caregivers was 24 hours per week, the average work time missed was 10.5 hours, mean absenteeism was 32%, mean presenteeism was 34.7%, and unadjusted mean work productivity loss was 51.2%. This study dealt with caregivers of paediatric patients. Since this study was based in Europe, where the average weekly work time is about 37 hours, it is difficult to compare with our study directly since the weekly worktime here is non uniform.
We also assessed the possible predictors of caregiver burden. Caregivers of 62% of Crohn’s patients and 52% of UC patients had significant burden. The p value here however was not significant. The study by Zand et al mentions a diagnosis of UC (rather than CD) as a risk factor for caregiver burden which is different from our observation. However, the number of UC patients in our study was too small to draw meaningful conclusions. We observed a higher percentage of caregiver burden in relation to: -
1) Female gender of caregivers (66% of female caregivers experienced significant burden compared to 51% in male counterparts)
2) Relationship with the patient- burden being more in parents (64% of mothers and 61.5% of fathers) compared to others (50% of spouses and 0% of siblings)
3) Lower education levels (64% of those educated up to tenth experienced burden while burden was 36% in those who were graduates or post graduates)
4) Longer disease duration- burden in 46% of those with disease duration one year compared to 63% in those with duration more than 1 year
5) Severe disease at presentation - burden in 76% of Crohn’s patients with CDAI≥ 221 at presentation compared with 44% in those with CDAI ≤220 at the time of initial diagnosis
6) Active disease at the time of interview- burden in 65% of caregivers of those with active disease at the time of interview compared to 56% in caregivers of those in remission
7) Use of biologicals- burden in 54% of caregivers of patients not on biologicals compared with 65% in those on biologicals
8) Percentage work hours missed (absenteeism)
9) Percentage impairment while working (presenteeism)
10) Percentage activity impairment
11) Percentage overall work impairment (work productivity loss)
Of these associations, initial disease severity, absenteeism, presenteeism, percentage activity impairment, work productivity loss showed a statistically significant association with caregiver burden.
Study by Parekh identified female gender, younger age, lower income, and history of psychiatric illness in the caregiver as predictors of caregiver burden while study by Zand et al, identified a diagnosis of UC, IBD disease activity and absenteeism to be greatly associated with caregiver burden similar to our study.
Attempts to improve caregiver wellbeing can have significant impacts in the treatment of IBD. Financial aids, support groups, counselling sessions regarding better coping strategies, behavioural interventions, prevention of addictions, subsidised medications and better health insurance schemes are a need of the hour.
5. Limitations
As the study was held at a tertiary care level referral centre, the patients may have had an overall severe disease, and hence it may not be possible to extrapolate the caregiver burden data and percentages to the general population.
Small sample size and disproportionate inclusion of CD and UC patients may have led to non-uniformity.
Being a cross-sectional study, follow up and changes in the burden level were not studied.
The tools used to measure burden were subjective questionnaires, hence an objective assessment may not have been possible.
6. Conclusions
To conclude, caregiver burden is a major problem area in the management of IBD patients and a vast majority of caregivers experience burden.
There is significant work hours missed, absenteeism, presenteeism and work productivity loss among working caregivers of young IBD patients.
There is statistically significant association of caregiver burden with initial disease severity, absenteeism, presenteeism, percentage activity impairment and work productivity loss.
Female caregivers, parents, caregivers of patients on biologicals, those with active disease during interview, longer disease duration and caregivers with lower education were found to have higher burden but these associations were not statistically significant.
Abbreviations
ASA | Aminosalicylic Acid |
ATT | Anti Tuberculosis Treatment |
CD | Crohn’s Disease |
CDAI | Crohn’s Disease Activity Index |
CRP | C Reactive Protein |
DA | Disease Activity |
ESR | Erythrocyte Sedimentation Rate |
FCP | Fecal Calprotectin |
IBD | Inflammatory Bowel Disease |
IFX | Infliximab |
QOL | Quality of Life |
TLW | Truelove Witts Score |
UC | Ulcerative Colitis |
WPAI | Work Productivity and Activity Impairment |
ZBI | Zarit Burden Interview |
Author Contributions
Remya Puthiya Veetil: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Sunil Kumar Kandiyil: Supervision, Validation, Visualization, Writing – review & editing
Sithara Balagopal: Supervision
Saji Sebastian: Supervision
Srijith Kadavanoor: Supervision
Funding
Authors declare that no funds, grants, or other support were received during the preparation opf this manuscript.
Data Availability Statement
The data used and analysed is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Philip M, Augustine P, Thomas V, Ramesh GN, Vinayakumar KR, Ramachandran TM, et al. Multi-center prospective survey of inflammatory bowel diseases in Kerala: More than 2000 cases. Indian J Gastroenterol. 2017 Nov 1; 36(6): 459-67.
|
| [2] |
Adolescence | Definition, Characteristics, & Stages | Britannica [Internet]. [cited 2022 Dec 5]. Available from:
https://www.britannica.com/science/adolescence
|
| [3] |
Lönnfors S, Vermeire S, Greco M, Hommes D, Bell C, Avedano L. IBD and health-related quality of life — Discovering the true impact. Journal of Crohn’s and Colitis. 2014 Oct; 8(10): 1281-6.
|
| [4] |
Zand A, Kim BJ, van Deen WK, Stokes Z, Platt A, O’Hara S, et al. The effects of inflammatory bowel disease on caregivers: significant burden and loss of productivity. BMC Health Services Research. 2020 Jun 18; 20(1): 556.
|
| [5] |
Shukla R, Thakur E, Bradford A, Hou JK. Caregiver Burden in Adults with Inflammatory Bowel Disease. Clin Gastroenterol Hepatol. 2018 Jan; 16(1): 7-15.
|
| [6] |
Guilfoyle SM, Denson LA, Baldassano RN, Hommel KA. Paediatric parenting stress in inflammatory bowel disease: application of the Pediatric Inventory for Parents. Child Care Health Dev. 2012 Mar; 38(2): 273-9.
|
| [7] |
Greenley RN, Cunningham C. Parent quality of life in the context of pediatric inflammatory bowel disease. J Pediatr Psychol. 2009 Mar; 34(2): 129-36.
|
| [8] |
Burke PM, Neigut D, Kocoshis S, Chandra R, Sauer J. Correlates of depression in new onset pediatric inflammatory bowel disease. Child Psychiatry Hum Dev. 1994; 24(4): 275-83.
|
| [9] |
Kahn SA, Lin CW, Ozbay B, Wang A, Chao J, Skup M. Indirect Costs and Family Burden of Pediatric Crohn’s Disease in the United States. Inflammatory Bowel Diseases. 2017 Dec 1; 23(12): 2089-96.
|
| [10] |
Klomberg RCW, Aardoom MA, Kemos P, Rizopoulos D, Ruemmele FM, Croft NM, et al. High Impact of Pediatric Inflammatory Bowel Disease on Caregivers’ Work Productivity and Daily Activities: An International Prospective Study. J Pediatr. 2022 Jul; 246: 95-102. e4.
|
| [11] |
Banerjee R, Pal P, Hilmi I, Raghunathan N, Rahman M, Limsrivillai J, Kamani L, Ghoshal UC, Aye TT, Joshi N, Alavinejad P, Peddi K, Patel R, Godbole S, Reddy DN. Primary caregiver burden and undiagnosed mental health illness in out-patients with inflammatory bowel disease-A multicentric prospective survey from the IBD Emerging Nations' Consortium. Indian J Gastroenterol. 2024 Dec; 43(6): 1156-1167.
https://doi.org/10.1007/s12664-024-01617-y
Epub 2024 Jul 18.
|
| [12] |
Bédard M, Molloy DW, Squire L, Dubois S, Lever JA, O’Donnell M. The Zarit Burden Interview: a new short version and screening version. Gerontologist. 2001 Oct; 41(5): 652-7.
|
| [13] |
Mc R, As Z, Em D. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics [Internet]. 1993 Nov [cited 2022 Nov 8]; 4(5). Available from:
https://pubmed.ncbi.nlm.nih.gov/10146874/
|
| [14] |
Akobeng AK, Miller V, Firth D, Suresh-Babu MV, Mir P, Thomas AG. Quality of life of parents and siblings of children with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 1999 Apr; 28(4): S40-42.
|
| [15] |
Loftus EV, Sandborn WJ. Epidemiology of inflammatory bowel disease. Gastroenterol Clin North Am. 2002 Mar; 31(1): 1-20.
|
| [16] |
Makharia GK, Ramakrishna BS, Abraham P, Choudhuri G, Misra SP, Ahuja V, et al. Survey of inflammatory bowel diseases in India. Indian J Gastroenterol. 2012 Dec; 31(6): 299-306.
|
| [17] |
Wang YF, Zhang H, Ouyang Q. Clinical manifestations of inflammatory bowel disease: East and West differences. J Dig Dis. 2007 Aug; 8(3): 121-7.
|
| [18] |
Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980 Dec; 20(6): 649-55.
|
| [19] |
Parekh NK. Effects of caregiver burden on quality of life and coping strategies utilized by caregivers of adult patients with inflammatory bowel disease. aog [Internet]. 2016 [cited 2024 Jul 28]; Available from:
http://www.annalsgastro.gr/files/journals/1/earlyview/2016/ev-09-2016-08-AG2759-0084.pdf
|
| [20] |
Psychosocial morbidity in prostate cancer: II. A comparison of patients and partners - PubMed [Internet]. [cited 2024 Jul 28]. Available from:
https://pubmed.ncbi.nlm.nih.gov/11069410/
|
| [21] |
Assessing the quality of life of household members of patients with inflammatory bowel disease: development and validation of a specific questionnaire - PubMed [Internet]. [cited 2024 Jul 28]. Available from:
https://pubmed.ncbi.nlm.nih.gov/12094861/
|
| [22] |
Gray WN, Graef DM, Schuman SS, Janicke DM, Hommel KA. Parenting Stress in Pediatric IBD: Relations with Child Psychopathology, Family Functioning, and Disease Severity. Journal of Developmental & Behavioral Pediatrics. 2013 May; 34(4): 237-44.
|
Cite This Article
-
APA Style
Veetil, R. P., Kandiyil, S. K., Balagopal, S., Sebastian, S., Kadavanoor, S. (2025). Caregiver Burden and Work Productivity Loss in Caregivers of Young Patients with Inflammatory Bowel Disease. International Journal of Gastroenterology, 9(2), 94-102. https://doi.org/10.11648/j.ijg.20250902.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Veetil, R. P.; Kandiyil, S. K.; Balagopal, S.; Sebastian, S.; Kadavanoor, S. Caregiver Burden and Work Productivity Loss in Caregivers of Young Patients with Inflammatory Bowel Disease. Int. J. Gastroenterol. 2025, 9(2), 94-102. doi: 10.11648/j.ijg.20250902.12
Copy
|
Download
AMA Style
Veetil RP, Kandiyil SK, Balagopal S, Sebastian S, Kadavanoor S. Caregiver Burden and Work Productivity Loss in Caregivers of Young Patients with Inflammatory Bowel Disease. Int J Gastroenterol. 2025;9(2):94-102. doi: 10.11648/j.ijg.20250902.12
Copy
|
Download
-
@article{10.11648/j.ijg.20250902.12,
author = {Remya Puthiya Veetil and Sunil Kumar Kandiyil and Sithara Balagopal and Saji Sebastian and Srijith Kadavanoor},
title = {Caregiver Burden and Work Productivity Loss in Caregivers of Young Patients with Inflammatory Bowel Disease
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {2},
pages = {94-102},
doi = {10.11648/j.ijg.20250902.12},
url = {https://doi.org/10.11648/j.ijg.20250902.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250902.12},
abstract = {Background: Inflammatory bowel disease (IBD) is associated with frequent hospitalizations, significant disability and impairment of quality of life. This can affect the physical, mental and overall wellbeing of not just the patients, but also the people caring for them. The aim of this study was to estimate the prevalence of burden among caregivers of young IBD patients, assess their work productivity impairment and identify the factors affecting caregiver burden. Methods: Design: This was a cross-sectional study conducted over a 16 month period at a tertiary care centre in north Kerala. Participants: 78 caregivers corresponding to 78 consecutive young IBD patients (aged 10- 24 years) were included. Two sets of questionnaires, the Zarit Burden Interview and the Work Productivity and Activity Impairment questionnaires tailored to suit IBD were used to assess burden and work productivity losses respectively. The study was approved by the institutional ethical committee. Results: A total of 78 caregivers, corresponding to 78 young IBD patients (aged 10- 24 years) were included in the study. 61 patients had Crohn’s disease and 17 patients had ulcerative colitis. Of the total number of caregivers, 47 caregivers (60.3%) experienced clinically significant caregiver burden. The mean ZBI score was 21.74± 10.3. The mean percentage work time missed (absenteeism) was 22.39%, the mean percentage impairment while working (presenteeism) was 40.0% and the mean percentage overall work impairment (loss of productivity) was 48.62%. Disease activity at the time of diagnosis (p=0.008 for Crohn’s p=0.002 for ulcerative colitis), absenteeism, presenteeism, work productivity loss and percentage activity impairment were significantly associated with caregiver burden Conclusion: Caregivers of young IBD patients experience significant burden and work productivity loss and this needs urgent attention to improve overall patient management.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Caregiver Burden and Work Productivity Loss in Caregivers of Young Patients with Inflammatory Bowel Disease
AU - Remya Puthiya Veetil
AU - Sunil Kumar Kandiyil
AU - Sithara Balagopal
AU - Saji Sebastian
AU - Srijith Kadavanoor
Y1 - 2025/08/11
PY - 2025
N1 - https://doi.org/10.11648/j.ijg.20250902.12
DO - 10.11648/j.ijg.20250902.12
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 94
EP - 102
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20250902.12
AB - Background: Inflammatory bowel disease (IBD) is associated with frequent hospitalizations, significant disability and impairment of quality of life. This can affect the physical, mental and overall wellbeing of not just the patients, but also the people caring for them. The aim of this study was to estimate the prevalence of burden among caregivers of young IBD patients, assess their work productivity impairment and identify the factors affecting caregiver burden. Methods: Design: This was a cross-sectional study conducted over a 16 month period at a tertiary care centre in north Kerala. Participants: 78 caregivers corresponding to 78 consecutive young IBD patients (aged 10- 24 years) were included. Two sets of questionnaires, the Zarit Burden Interview and the Work Productivity and Activity Impairment questionnaires tailored to suit IBD were used to assess burden and work productivity losses respectively. The study was approved by the institutional ethical committee. Results: A total of 78 caregivers, corresponding to 78 young IBD patients (aged 10- 24 years) were included in the study. 61 patients had Crohn’s disease and 17 patients had ulcerative colitis. Of the total number of caregivers, 47 caregivers (60.3%) experienced clinically significant caregiver burden. The mean ZBI score was 21.74± 10.3. The mean percentage work time missed (absenteeism) was 22.39%, the mean percentage impairment while working (presenteeism) was 40.0% and the mean percentage overall work impairment (loss of productivity) was 48.62%. Disease activity at the time of diagnosis (p=0.008 for Crohn’s p=0.002 for ulcerative colitis), absenteeism, presenteeism, work productivity loss and percentage activity impairment were significantly associated with caregiver burden Conclusion: Caregivers of young IBD patients experience significant burden and work productivity loss and this needs urgent attention to improve overall patient management.
VL - 9
IS - 2
ER -
Copy
|
Download